|
Anapafseos 5 Agios Nikolaos 72100,Crete,Greece,00302841026182,00306932607174,alsfakia@gmail.com
Blog Archive
- ► 2022 (3010)
- ► 2021 (9899)
-
▼
2020
(4138)
-
▼
December
(1380)
-
▼
Dec 10
(86)
- Sexual Dimorphism in Colon Cancer
- Microbiome Related Cytotoxically Active CD8+ TIL A...
- Cone-Beam-CT Guided Adaptive Radiotherapy for Loca...
- Development and Validation of a Nomogram for Diffe...
- Chinese Herbal Medicine for Reducing Chemotherapy-...
- Role of Specific B-Cell Receptor Antigens in Lymph...
- Reconstruction of Immune Microenvironment and Sign...
- Microsurgical Lymphedema Treatment:
- Morning serum cortisol is superior to salivary cor...
- The role of the superior parietal lobule in lexica...
- Enhanced recovery after breast reconstruction with...
- Brain MRI post-processing with MAP07 in the preope...
- Surgical management of the fourth ventricular tumo...
- FAM46A expression is elevated in glioblastoma and ...
- Delayed transhemispheric propagation of electrogra...
- Early-Onset Autosomal Recessive Spastic Ataxia of ...
- Papillary Tumor of the Pineal Region in Pediatric ...
- Reconstruction of chronic scalp erosion after deep...
- A Study of TAR-200 in Combination With Cetrelimab ...
- Triamcinolone Levels in Cochlear Perilymph, Latera...
- The Effect of Non-resistance Technique for Neck Pa...
- Ramucirumab and Trifluridine/Tipiracil or Paclitax...
- Study of Pharmacokinetic, Safety, Immunogenicity a...
- Acute Myeloid Leukemia: From Biology to Clinical P...
- MR-Guided Radiotherapy for Prostate Cancer
- The Accuracy of Different Modalities of Perforator...
- Analysis of N6-Methyladenosine Methyltransferase R...
- Prevalence of oral mucosal normal variations and l...
- Repurposing Cationic Amphiphilic Drugs and Derivat...
- Comprehensive Molecular Characterizations of Chine...
- A Hematological-Related Prognostic Scoring System ...
- Concurrent Genetic Alterations and Other Biomarker...
- Systematically Characterizing A-to-I RNA Editing N...
- Molecular Alterations in Metastatic Ovarian Cancer...
- Integrative Analysis of Multi-Omics Identified the...
- Identification of Novel MeCP2 Cancer-Associated Ta...
- Cadherins, Selectins, and Integrins in CAM-DR in L...
- Beyond TNBC: Repositioning of Clofazimine Against ...
- Neutrophils as Orchestrators in Tumor Development ...
- Qualitative MR Imaging Features for the Differenti...
- A Nomogram Based on Serum Biomarkers and Clinical ...
- Macrophages in Osteosarcoma Immune Microenvironmen...
- Stereotactic Body Radiation Therapy for Extracrani...
- Types of Mastectomies and Immediate Reconstruction...
- Cepharanthine induces the proliferation of human d...
- The Role of Hippocampal Neurogenesis in ANT-DBS fo...
- Efficacy of antimicrobial photodynamic therapy wit...
- Antimicrobial peptides for the prevention and trea...
- PET detectives: Molecular imaging for phaeochromoc...
- NR5A1 c.991‐1G > C splice‐site variant causes fami...
- Klotho gene G395A and C1818T polymorphisms in acro...
- The use of growth hormone therapy in adults with P...
- Oxytocin in young children with Prader‐Willi syndrome
- Association of urinary free cortisol with bone for...
- SRY‐negative 46,XX testicular/ovotesticular DSD: l...
- Classification and morphology of middle mesial can...
- Peroneal Flap – How to Harvest and Clinical Apprai...
- Inferior Alveolar Nerve Reconstruction in Extensiv...
- Technical Principles and Clinical Workflow of Tran...
- The human melanocyte and melanoblast populations p...
- Efficacy and Safety of Mesenchymal Stem Cell Clust...
- Efficacy and Safety of Pembrolizumab (MK-3475) Plu...
- Pilot Study of a 1-Millimeter Resolution Clinical ...
- Systemic Inflammation Response Index Is a Predicto...
- Retention and survival rate of etanercept in psori...
- The Goldman‐Fox Syndrome: Treating and Preventing ...
- Evaluation of lens clarity in children with atopic...
- Antimicrobial photodynamic therapy in the treatmen...
- Increased risk of depression and impairment in qua...
- Scrotal erythema and geographic tongue subsequent ...
- Dermoscopic characterization of guttate psoriasis,...
- Skin manifestations in SARS‐CoV‐2 infection
- Topical and Systemic Retinoids for the Treatment o...
- Evaluation of Oral Isotretinoin Effects on Hearing...
- Losartan for treatment of epidermolysis bullosa – ...
- investigation of thyroid blood tests and thyroid u...
- Rituximab in Practice: Clinical Evaluation of Pati...
- The Most Common Allergens
- The risk for severe COVID 19 in patients with auto...
- Hypertrichosis and hair repigmentation in patients...
- Adalimumab in the management of hidradenitis suppu...
- Unsuccessful palliative treatment of extraocular s...
- Ectropion surgery might not be a long‐term solutio...
- Can Rituximab Be Used In The Treatment Of Pemphigu...
- The additive efficacy of therapeutic low‐intensity...
- Safety and efficacy profile of oral cyclosporine v...
-
▼
Dec 10
(86)
-
▼
December
(1380)
- ► 2019 (2429)
Αλέξανδρος Γ. Σφακιανάκης
Thursday, December 10, 2020
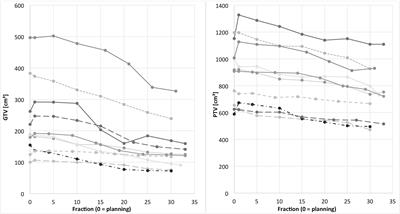
Cone-Beam-CT Guided Adaptive Radiotherapy for Locally Advanced Non-small Cell Lung Cancer Enables Quality Assurance and Superior Sparing of Healthy Lung
Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment