In this article, we're going to take a deep dive into hydroxyapatite. We'll cover what it is, how beneficial it is to help stop tooth decay, and the potential risks of nano-hydroxyapatite.
Fair warning, this article is going to be a deep dive that provides a lot of details about hydroxyapatite.
So if you're new here and you'd like a more high-level introduction to remineralization or hydroxyapatite's role in helping to stop and/or protect against tooth decay, these articles may be an easier read:
In 2016, we launched our Shine Remineralizing Tooth Whitening Powder, which contains naturally sourced hydroxyapatite (it's actually the #1 ingredient in Shine  ). Since then, many other companies have developed oral hygiene products using various forms of hydroxyapatite.
). Since then, many other companies have developed oral hygiene products using various forms of hydroxyapatite.
It makes sense that hydroxyapatite's popularity is on the rise. After all, the research clearly shows that hydroxyapatite protects against tooth decay just as well as (and sometimes even better than) fluoride.
However, like so many things in life, not all hydroxyapatites are created equal. The quality, quantity, and particle size of a product's hydroxyapatite can all make a big difference.
Speaking of particle size, the blogosphere has recently been abuzz with debates about the risks vs. benefits of nano-sized hydroxyapatite. So, we decided to provide more information so you can make up your own mind on this developing subject.
What is hydroxyapatite?
To start, let's make sure we're all on the same page.
Hydroxyapatite (high-drox-ee-appetite), is the chemical name for a molecule made up of calcium, phosphorus, oxygen, and hydrogen. For you scientists (or armchair scientific types, like me), the chemical composition is Ca5(PO4)3OH. However, since it shows up as a pair in nature, it's commonly notated as Ca10(PO4)6(OH)2. The word 'hydroxyapatite' is commonly abbreviated as HA.
The HA molecule is very important for oral care.
It's the primary building block that our teeth are made of.
But for decades, instead of focusing on hydroxyapatite, we've been taught that we need to use fluoride to prevent tooth decay. Leaning on our high school chemistry class, we might recall that fluoride is a halide, which means it's a super 'attractive' element.
When we introduce fluoride into the mouth, it binds with the calcium and phosphorus components of our teeth, which creates fluorapatite (note, not hydroxyapatite). However, our teeth do not naturally contain fluoride, and tooth decay is not the result of a fluoride deficiency.
So, for the purposes of this article, we'll set aside fluoride. Instead, we'll anchor on the fact that our teeth are made of hydroxyapatite, which is why HA is such a supportive compound for tooth health.
Quick primer on particle size…
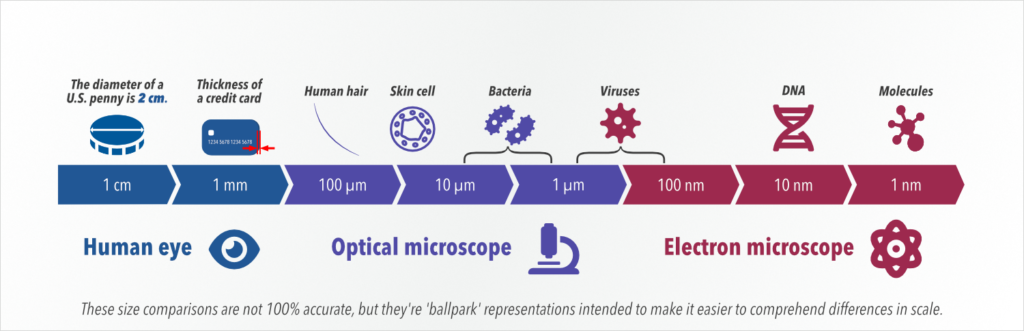
Particle sizes can be expressed using different units of measurement. For the size we'll be dealing with here, the metric system is generally used. We'll be talking in micrometers (also called microns) and nanometers. And for perspective, let's zoom out and start with millimeters.
Millimeters are the tiniest marks on a standard US/metric ruler. 10 millimeters = 1 centimeter, which is about ⅓ of an inch.
(As a side note, if you've had a periodontal depth test, you probably know that the numbers the dentist calls out to the assistant are in millimeters. Any gum pocket that's deeper than 4 millimeters is problematic. Once gum pockets get deeper than that, it's difficult to effectively maintain healthy bacterial populations. Thankfully, there's a product solution that can help if you have deeper gum pockets. Now let's get back to measurements…)
There are 1000 micrometers in a millimeter.
Stepping down another rung into the hard-to-imagine range, there are 1000 nanometers in 1 micrometer.
So, that means that there are one million nanometers in one millimeter.
Here's the takeaway that will help simplify this: 'nano' is one thousand times smaller than 'micro'.
So for example, something that's 5 micrometers in diameter could also be measured as 5000 nanometers. In other words, nanoparticles are WAY smaller than microparticles.
To look at it another way, if a golf ball were one nanometer in diameter, a micrometer would be nearly half a football field in diameter, and one millimeter would be just over 23 miles. So, nanometers are 1000 times smaller than micrometers, which are 1000 times smaller than millimeters.
Particle size matters…
Hydroxyapatite can come in many different particle sizes. For medical, dental, and oral supplement applications, particle sizes range from about 800 micrometers all the way down to 10 nanometers (80,000 times smaller).
To assist with optimal uptake in the mouth, we want the particle size to be pretty tiny. That way, it can go into suspension with our saliva and be available to deposit more minerals into and onto our teeth. (For more info on how this works with Shine, please take a look at this video.)
The naturally sourced hydroxyapatite we use in Shine is pharmaceutical-grade bone powder from grass-fed New Zealand cattle.
(Incidentally, the same hydroxyapatite that we use is also used in the supplement field as a bioavailable source of calcium. In fact, there's substantial evidence that suggests that the body uptakes HA better than other forms of calcium.)
We use the finest particle size our team can mechanically produce, which is right around 70 micrometers. To differentiate it from nano-HA, we refer to our hydroxyapatite as MCHA (microcrystalline hydroxyapatite) with the 'micro' distinguishing the particle size of the HA.
But if a tiny size is better, why not use the smallest possible particle size?
As we go from micrometers to nanometers, we have to think about what might happen in the body if we use an ingredient with such a tiny particle size.
Nano or no-no?
If you've been reading our material for a while, you already know that OraWellness is hardwired to a holistic paradigm. This affects many of our decisions, especially when it comes to product development.
When we were doing the R&D for Shine, we saw that the research literature supported using nano-HA for helping to restore demineralized areas in teeth. But we also saw some bad PR about nano-sized particles indiscriminately traveling throughout the body (due to their extremely tiny particle size).
In our opinion, nano-HA had two things going against it:
- The particle size was so tiny that the molecule was able to easily migrate throughout the body (for example, across the blood-brain barrier and even into the cellular structure), and literature was emerging that suggested that this wasn't safe.
- Nanoparticles are synthetically produced (not naturally derived).
So, with our holistic paradigm guiding us, we chose to apply the 'precautionary principle' and avoid nano-HA until we knew for certain that it was safe to use long-term.
(For more info on our thought process in these situations, check out our simple, two-step exercise that you can apply to any hygiene product to determine if it's holistic or not.)
What are the risks with nano-HA?
In the EU, there's a General Product Safety Directive that says, "Businesses must only place products which are safe on the market…" But, nano-HA hasn't been proven to be safe.
In fact, earlier this year, the European Union announced that it plans to ban several nano-sized materials (including nano-HA) for use in cosmetic and oral hygiene applications. Here's a link to the full report on nano-HA from the EU's Scientific Committee on Consumer Safety (SCCS).
The SCCS is especially concerned about the potential for nano-HA to damage cell DNA. The term they reference is 'genotoxic potential', which means the possibility for something (in this case, nano-HA) to damage the genetic information within a cell, causing mutations that may lead to cancer.
In their report, the SCCS states, "Having considered the data provided, and other relevant information available in scientific literature, the SCCS cannot conclude on the safety of the hydroxyapatite composed of rod-shaped nanoparticles for use in oral-care cosmetic products at the maximum concentrations and specifications given in this Opinion. This is because the available data/information is not sufficient to exclude concerns over the genotoxic potential of HAP-nano."
And their hesitancy seems warranted for other reasons, too. Other studies point to issues like the risk that nano-HA may cause cellular breakdown in kidney cells and that it may even have a negative impact on human blood cells.
All of this provides plenty of reasons for us to continue to apply the precautionary principle and steer clear of nano-HA.
But what does the SCCS think about NON-nano-HA?
In section 3.3.4 Assessment of the systemic toxicity of the non nanoform of HAP, the report says, "Calcium phosphate is a common mineral on earth and the most common calcium phosphate mineral is hydroxyapatite. Calcium phosphates have been generally recognized as safe (GRAS) in food by the FDA in 1975. Calcium phosphate is highly biocompatible in contact with hard tissue because the body is well accustomed to this mineral."
Thank goodness we can still benefit from using hydroxyapatite without the risks of using nanoparticles.
Is microcrystalline HA as effective as nano-HA?
There are two ways science seeks to prove or disprove any hypothesis: via clinical trials or via empirical evidence (any patterns or behaviors found during personal observation or experimentation).
Let's start with what the research currently says about the efficacy of micro-HA.
To our knowledge, there are no research studies comparing different sizes of HA against one another. Here's a study that mentions both micro- and nano-HA, but we haven't yet found data that compares the efficacy of various particle sizes of HA.
However, here's a well-done study that compares micro-HA to the gold standard of conventional dentistry: 1400 ppm (particles per million) fluoride. The researchers chose to study individuals with braces (which is a group that's at high risk for decay). Here's the takeaway:
"In highly caries-active patients, the impact of the regular use of a microcrystalline HAP dentifrice [toothpaste] on caries [cavities] progression is not significantly different from the use of a 1400 ppm fluoride toothpaste."
At first blush, that might not sound very noteworthy. But, the data in that study actually shows that the participants who used a micro-HA toothpaste had less decay than those who used a fluoride-based toothpaste.
And, this one-year, double-blinded, randomized controlled trial tested whether micro-HA protects children against early cavities as effectively as fluoride-based toothpaste. It found, "This RCT [randomized controlled trial] showed for the first time, that in children, the impact of the daily use of a toothpaste with microcrystalline hydroxyapatite on enamel caries progression in the primary dentition is not inferior to a fluoride control toothpaste."
And what about empirical evidence?
Well, we have plenty of that from the thousands of testimonials we've received from you, our community, through the years since we launched Shine, our remineralizing tooth whitening powder with MCHA.
We love all of the testimonials we regularly receive. Some of them are jaw-droppers, like this one:
"I just found out one of the reasons I struggled with cavities for years: I have an autoimmune disease which causes dry mouth, and was depleted by stress and further health issues. I ended up with 11 cavities a few years ago despite great oral hygiene. I finally ordered many of your products at that time, including several containers of Shine.
Within 3 months, 10 of the cavities were gone and only the oldest deepest one needed a filling. The hygienist thought I must have had those cavities filled elsewhere as they were gone.
I have continued to use your products, and in the 3 years since then, have no new cavities, continued great gum health, and very little plaque at my dental visits. I love the smooth feel of the oil blend on my teeth, and it feels good to know that I can prevent cavities despite this autoimmune condition. Thank you!"
– Tara B. from Canada< /h2>
This is empirical evidence, plain and simple. And we're honored that so many of you have used our product solutions to create greater oral health for yourself. That's dental self-empowerment.
Wrapping up…
Thanks for joining us for this fascinating deep dive on hydroxyapatite and particle sizes. For more information on hydroxyapatite as well as other in-the-mouth and whole-body strategies for helping teeth remineralize, feel free to download our free eBook, How to Stop Tooth Decay and Remineralize Your Teeth.
What about you, what are your thoughts on nano- vs. microparticles? Are the benefits of using nano-HA greater than the risks? Ultimately, it becomes a personal value judgment. We hope this information helps you to make educated decisions on what ingredients to use in your oral hygiene strategy. Please share your thoughts and experiences in the comments below so we can all learn from each other.
Helpful, related resources:
Other resources:
The post Nano or No-No? Hydroxyapatite Particle Size Matters… appeared first on OraWellness.